The TPLO-M surgery - description of the procedure for a 2.0 non-locking TPLO-M plate
The stifle of a 5.5 kg 10+ old yorkshire terrier dog was operated last week due to a grade 3/4 medial patella-luxation and cranial cruciate ligament rupture. The modified TPLO surgery (TPLO-M) and the recently developed Smartvet TPLO-M mini (terraced) plate are excellent for the simultaneous treatment of lesions.
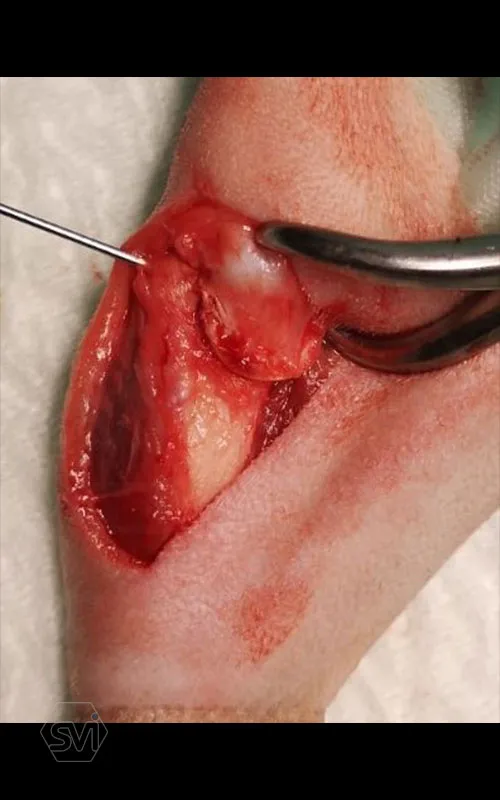
During the operation, the joint was first opened by parapatellar lateral arthrotomy, and the significantly worn and shallow patellar groove was deepened, and the excised cartilage piece was reinsert. To deepen the groove, we used the SMARTVET mini oscillating saw with a narrow, thin blade ideal for this task. A review of the deeper layers of the joint found the meniscus intact, leaving them in place. The lateral part of the joint capsule was narrowed by the “over the top” suture technique, while the medial part was loosened by parapatellar incision.
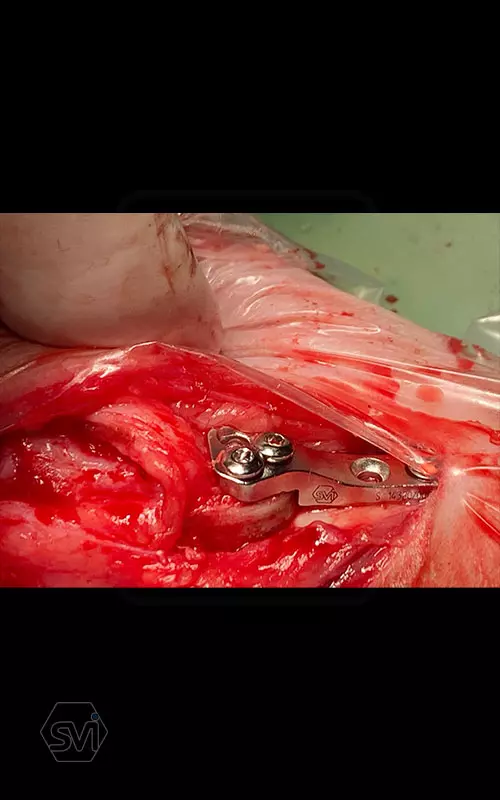
The next step was an osteotomy with a curved saw using an R12 blade and a Smartvet cordless TPLO saw. Since no JIG is used for the operation, the excised bone piece was grasped with a small pointed condylus forceps (small-spitzige) and adjusted to the desired position by the sterile assistant: that an approx. a 2 mm step should be created. This position was fixed with a 1.0 mm K-wire starting from the proximal end of the tuberositas tibiae. The TPLO-M mini plate was used, with a minimal bend, the proximal piece was curved outward for a better fit. The terraced design of the plate was aligned with the 2.2mm step to the bone. Screw insertion order: proximal middle and cranial holes, then distal middle DCP holes (INTRAOP. PICTURE) The three screws were tensioned continuously and alternately, and the temporaly K-wire was removed, thus providing the opportunity for the displacement to be complete and for the osteotomized tibia to assume the position formed by the plate and for compression to develop between bone surfaces. The other screws were then inserted. In our case, the K-wire was no longer returned. (If there is place and way for it, we can put it back a few tenths of a millimeter thicker than the previous one taken out to relieve the crista tibiae. tibiae may break under the load.)
Moving the knee, the patella could no longer be luxated, and the ligamentum patellae straightened and moved in the middle line of the jont.
Further information: This email address is being protected from spambots. You need JavaScript enabled to view it., www.smartvetimplats.com
Egy friss TPLO-M műtét – a műtét menetének leírása 2.0 DCP furatos TPLO-M lemez esetén
5,5 kg-os idős yorki kutyának a térdét operáltuk tegnap, grade 3/4-es mediális patella-ficam és elülső kereszteződő-szalag szakadás miatt. Az elváltozások egyidejű ellátására kiválóan alkalmas a módosított TPLO műtét (TPLO-M), és az ehhez fejlesztett Smartvet TPLO-M mini (teraszos) lemez.
A műtét során először az ízületet nyitottuk ki, parapatellaris lateralis arthrotomiával, a jelentősen megkopott és sekély ízületi árkot mélyítettük a kivésett porcdarab visszaillesztésével. Az árok mélyítésére a mini oszcillációs fűrészt használtunk, amely keskeny, vékony pengéje ideális erre a feladatra. Az ízület mélyebb rétegeinek áttekintése során a meniscusokat épnek találtuk, így azokat helyben hagytuk. Az izületi tok lateralis részét „over the top” technikával szűkítettük, míg a medialis részen parapatellaris metszéssel lazítottuk.
A következő lépés az ívelt fűrésszel való oszteotomia volt, R12 pengét használtunk, és Smartvet akkumlátoros fűrészt. Mivel JIG-et nem használunk a műtéthez, a kivágott csontdarabot kisméretű hegyes condylus-fogóval (kis-spitzige) megragadtuk, és a steril asszisztens a kívánt pozícióba állította: egyrészt a TPA-nak megfelelően elforgatva, majd medialis irányba kiemelve kissé tibia síkjából úgy, hogy egy kb. 2 mm-es lépcső keletkezzen. Ezt a pozíciót egy 1,0 mm -es K szeggel rögzítettük a tuberositas tibiae proximális végétől indítva. A TPLO-M mini lemezt használtuk, egy minimális hajlítással a proximális darabot kifelé görbítettük a jobb illeszkedés végett. A lemez teraszos kialakítását a lépcsőhöz igazítottuk (2,2 mm-es eltolás), és így pozícionáltuk a lemezt. A csavarok behelyezési sorrendje: proximális darab középső és cranialis furat, majd a distalis darab középső DCP furat (INTRAOP. KÉP) A három csavart folyamatosan, felváltva feszítettük, majd a végállapot előtt a pozíciót rögzítő K-szeget a tub. tibiae-ből eltávolítottuk, ezzel biztosítottuk a lehetőségét annak, hogy az eltolás teljes legyen és az oszteotomizált tibia felvegye a lemez által kialakított pozíciót, illetve, hogy kialakuljon a kompresszió csontfelszínek között. A többi csavar behelyezése ezután következett. Esetünkben a K-szeget már nem tettük vissza. (Abban az esetben, ha van hely és mód rá, akkor a kivett előző szegnél néhány tized milliméterrel vastagabbat visszahelyezhetünk a crista tibiae tehermentesítése céljából. Itt ügyelni kell, hogy a szeg soha se menjen a patella egyenes szalagjának tapadási pontja alá, mert a tub. tibiae letörhet a terhelés hatására.)
A térdet átmozgatva a patella már nem volt ficamítható, az egyenes szalagja pedig kiegyenesedett és az ízület középső síkjában mozgott.
További információ: This email address is being protected from spambots. You need JavaScript enabled to view it., www.smartvetimplats.com
The TPLO-M surgery - description of the procedure for a 2.0 non-locking TPLO-M plate - image gallery




Would you like
to buy?
Do you have a question?



Hits: 1013